29-06-2020
COVID-19 and cruise ships: A drama anounced
Angela Teberga | Alba Sud
Photography by: Cristian Ruz, under creative commons license.
“The history repeats itself, the first time as a tragedy and the second as a farce”
(Karl Marx in The Eighteenth Brumaire of Louis Napoleon)
The imminent spread of infectious and contagious diseases within a ship has always been a cause of tension among sailors, and a challenge that is difficult to resolve for professionals of health control. It is a reason for tension among the crew because, being away from their homes, they fear becoming ill and not receiving appropriate specialized medical treatment. And it is also a challenge in the order of health control because the confinement, together with the high concentration of people in a single space, enhances the transmission of diseases among those on board, requiring strict control protocols by the health authorities and prevention programs by the cruise industry.
Some people compare a ship with a “petri dish”, a cylindrical container used in the laboratory for the cultivation of microorganisms, since both would function as incubators for microbes and, therefore, ideal vehicles for the spread of diseases. It is not by chance that news of viral and bacterial diseases is frequently circulated in the mainstream media. Only among Brazilian crew members, we are aware of cases or outbreaks of scabies (2011), gastroenteritis (2011), H1N1 (2012), measles (2019) and, more recently, COVID-19 - which we will talk about it in this article.
What does the international literature say about it?
In international literature, we find specific articles in medical journals about the occurrence of communicable diseases, among passengers and crew, on cruise ships. Mouchtouri et al. (2010) cite the occurrence of outbreaks and/or infections in vessels by, especially, legionella, salmonella, escherichia coli, vibrio (bacteria) and norovirus, influenza A and B (virus). Pavli et al. (2016) state that the majority of infections registered on cruise ships are respiratory (29%) and gastrointestinal (10%).
Fujita et al. (2018) analyzed the notifications, systematized by the National Health Surveillance Agency (ANVISA), of communicable diseases on board cruise ships on the Brazilian coast, in the period between 2009 and 2015. The analysis of the notifications indicate that norovirus was the main etiologic agent of the outbreaks of that period, although the rate of outbreaks has decreased over time. The authors conclude that the large number of passengers and crew confined to ships would be the main reason for the contamination. “This represents a high potential risk for the transmission of infectious diseases due to the confinement of these travelers in common spaces, with a high probability of exposure to fomites by the oscillation of the vessel” (Fujita et al., 2018, p. 11). They cite mini-cruises (that is, cruises with short routes of 3 to 4 days) as a problem for the control and supervision of epidemiological outbreaks, as it is common for communicable diseases to have an incubation time longer than the duration of the trip itself.
Fernandes et al. (2014), in a study on the outbreak of Influenza B on a cruise ship off the coast of the state of São Paulo, in February 2012, concluded that crew members housed on the two lower decks were more likely to develop symptoms of illness similar to influenza (fever, cough, sore throat and dyspnea). The conclusion is related to confinement and the absence of air circulation, according to the authors.
The lower-ranking crew members were on such decks, usually sharing cabins that fit two to four people. There were no windows and circulated air came from air conditioners. The influenza virus is spread through droplets and aerosol from infected people when coughing and sneezing. Closed and crowded places, such as the ship’s lower decks, facilitate the spread of influenza virus (Fernandes et al., 2014, p. 301).
Mitruka et al. (2012) explains that outbreaks on cruise ships of vaccine-preventable diseases, such as rubella, chickenpox and measles, are associated with the introduction and spread among crew members from countries with endemic transmission of these diseases, in addition to low rates of vaccination or not introduced or recently introduced the vaccine. Again, the confined and densely populated environment is cited as a facilitator of the transmission of contagious diseases, including vaccine-preventable diseases.
Kak (2015) remembers that “an infectious agent introduced into the environment of a cruise ship has the potential to be distributed widely across the ship and to cause significant morbidity”. The infectious pathogens of potential risk in cruise ships can be, according to the author, gastrointestinal, respiratory and skin. One of the reasons for the high morbidity (rate of carriers of a certain disease in relation to the total population studied, in a given location and at a given time) within ships would also be related to the average age of passengers on ships, over 45 years old, and usually with chronic medical problems.
Finally, we highlight the important research by Zheng et al. (2016) on the transmission of respiratory diseases on passenger ships. The authors begin the article by remembering that, although the voyage by ship supposes an outdoor experience, passengers and crew are mostly indoors, such as restaurants, theaters, dance halls and the cabins themselves. In addition, they share public bathrooms, the same food and drinks, as well as the same air conditioning system. Finally, they recall that approximately one third of passengers are elderly people, who are more susceptible to infectious diseases than the rest of the population.
The authors state that outbreaks of respiratory diseases in passenger ships are aggravated by specific vulnerabilities of the ships, namely: a) a large number of people in close contact; b) duration of travel long enough to cover the period of virus transmission and incubation; c) diversity of people in the southern and northern hemisphere, where influenza vaccination may not be available during the disease season; and d) crew members can be continuous vehicles for transmitting the virus, as infections can remain on board a cruise from one trip to the next (Zheng et al., 2016).
The results of the study by Zheng et al. (2016) point out that the risk of infection by a crew member is higher than the risk of a passenger, because the crew member has contact with all the groups of the ship. They also indicate that the use of face masks by crew members serving in restaurants, bars or lounges, as well as the increase in the rate of air exchange in some or all locations on the ship, resulted in a moderate reduction in the rate of respiratory disease transmission. The most effective measure for reducing the transmission rate was the installation of high efficiency air filters and devices for germicidal ultraviolet irradiation in the ship's ventilation systems.
The articles cited in this introduction suggest that the prevention of communicable diseases on board ships necessarily involves:
- Strictness with sanitary conditions and sanitary control measures in ports and ships;
- Vaccination requirement for diseases preventable by vaccination between passengers and crew;
- Quarantine imperative for sick passengers and/or crew members, who must remain isolated in their cabins to avoid contagion among other passengers;
- Use of face masks and incentive to respiratory hygiene and cough etiquette;
- Installation of high efficiency air filters and germicidal ultraviolet irradiation devices in the ship's ventilation systems.
All the articles cited support the thesis that the confinement and concentration of people on cruise ships enhances the transmission of diseases. It cannot be said, therefore, that the shipowners were unaware of the imminent problem of contamination of some infectious and contagious disease, of any severity, between their passengers and crew. Unfortunately, an even more serious disease, discovered at the end of 2019, was found on several cruise ships in mid-February 2020. COVID-19, which spread to 188 countries and regions, has been diagnosed in more than 9 million of people and killed almost half a million people worldwide, according to monitoring by Johns Hopkins University, also reached the ships.
Cruise Ships and the COVID-19
COVID-19, a disease caused by the SARS-CoV-2 coronavirus, was discovered on December 31, 2019 after cases registered in Wuhan (China). On March 11, 2020, the World Health Organization (WHO) started to characterize it as a pandemic, due to the alarming levels of spread and severity of the disease, having reached almost all countries in the world. The danger of the disease is related to its high contagion power, even among asymptomatic infected people. The high transmissibility of the disease is even greater in confined spaces, according to Mizumoto & Chowell (2020), including hospitals, prisons, churches and, of course, cruise ships.
Between March 9 and 26, all major cruise lines suspended operations, voluntarily and temporarily, across their entire fleet. The main reasons for the downtime would have been: to avoid contagion of the new coronavirus between crew and passengers, in addition to the sudden drop in demand and operational instability.
However, most companies were slow to suspend operations in a few days, or even weeks, after the WHO statement that characterized the disease as a global pandemic. Images like this (Image 1) circulated on social networks and international newspapers: crew members working in the second half of March, when the disease was already present in almost the entire globe - on March 11, the date of the WHO declaration, there were 125 thousand people infected; on March 26, the date on which the last shipowner suspended its operations, the number more than quadrupled, from 529 thousand contaminated.
Image 1 - Philippine crew member working with improvised mask (22/March)

Philippine crew member working with improvised mask (22/March). Source: Comitato No Grandi Navi.
Table 1 shows the exact days when cruise ship operations are suspended. These are dates on which new passenger shipments were no longer carried out, and in several cases, the last passengers had to stay and carry out social isolation on board. That is because, in mid-March, countries like the United States of America, Canada, New Zealand and Australia banned passenger ships from docking at their ports, as required by local health control agencies.
The Zaandam ship, from Holland America company, for example, faced an emergency situation on board, with just over 100 shipped people with symptoms similar to those of COVID-19. The ship was in the Pacific Ocean and intended to cross the Panama Canal to land passengers on the east coast of the United States of America. Panamanian health control bodies, however, did not allow the ship to transit through the canal, only allowing the transfer of healthy passengers from Zaandam to another ship of the same company.
Several ships, such as the Costa Deliziosa, the MSC Magnifica and the Pacific Princess, remained in operation for weeks and even months, awaiting authorization to dock. On June 8, the Artania, the last cruise ship in operation, finally made its final stopover at the port of Bremerhavan (Germany), after six months of sailing.
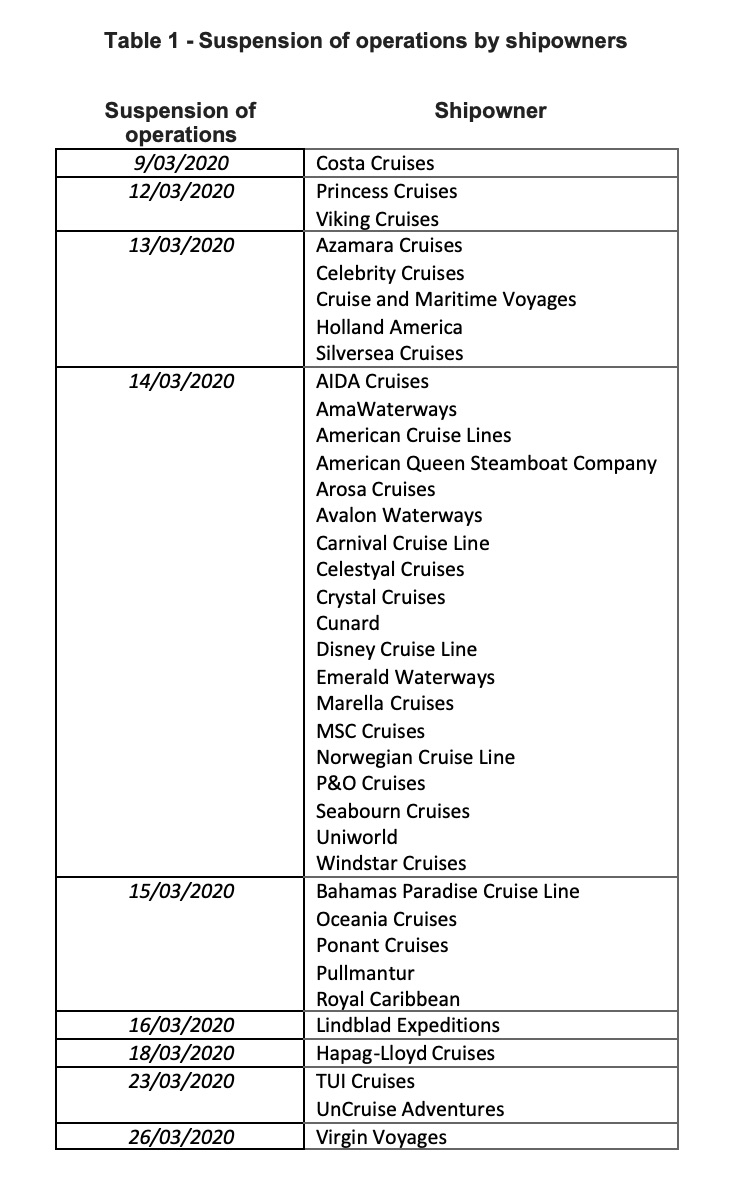
Source: Organized from data from Cruise Mapper.
Unfortunately, the new disease was seen on several cruise ships as early as mid-February 2020. It is reported that more than 3,200 people (including passengers and crew) were infected with COVID-19 inside the ships, of which more than 70 died. In image 2, it is possible to verify the mapping, carried out between January and March 2020, of cruise ships with cases of COVID-19.
Image 2 - Cruise ships with cases of COVID-19 (January to March 2020)

Source: Centers for Disease Control and Prevention.
An expressive number of cases/outbreaks by the disease have been recorded on several cruise ships around the world. Table 2 shows the number of positive tests for the new coronavirus among crew and passengers per ship, including the number of deaths.
Table 2 - Cases/outbreaks of contamination by the new coronavirus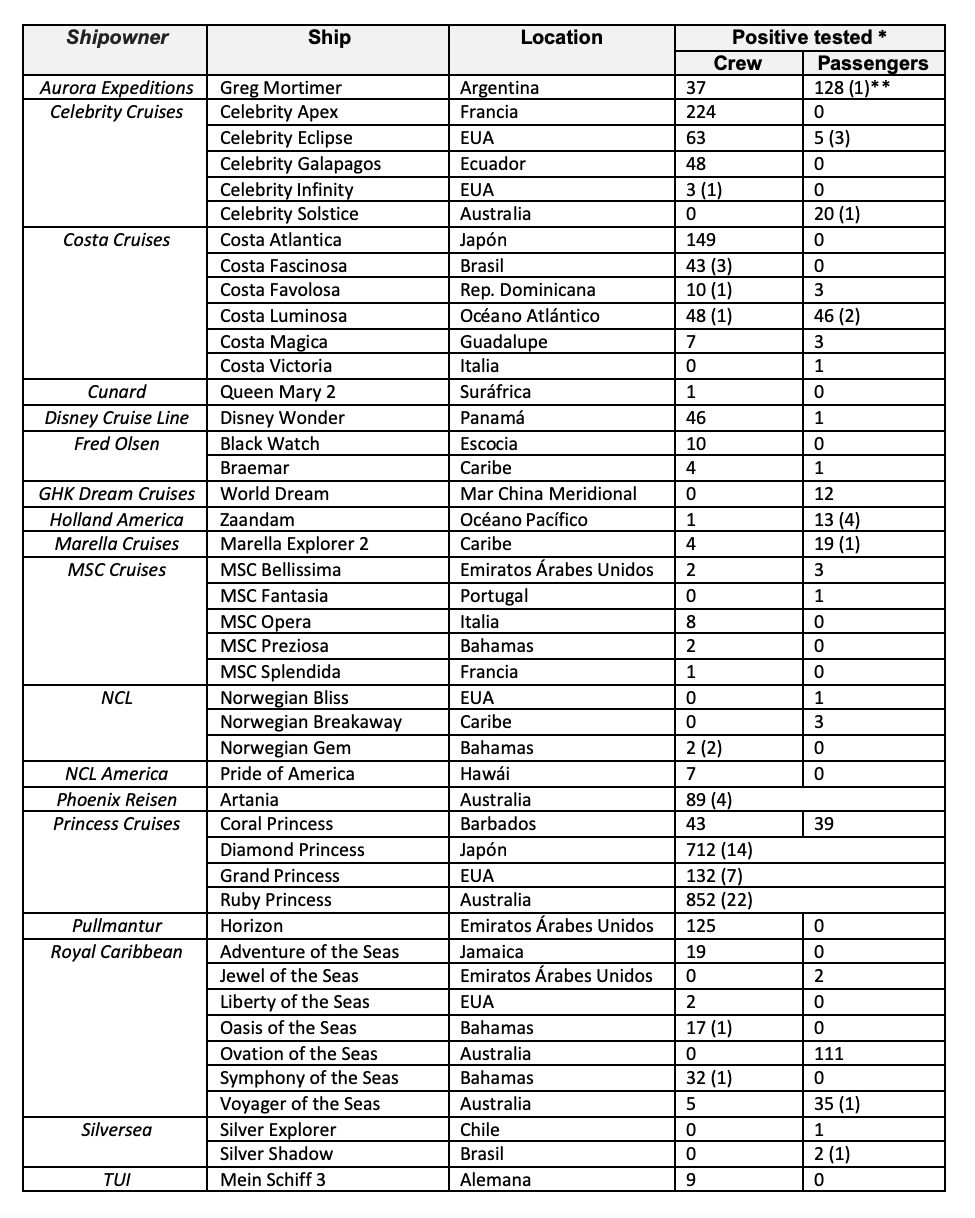
Source: Organized from data from Cruise Mapper.
As shown in the spreadsheet, the two largest coronavirus outbreaks occurred on the Ruby Princess ships (March | Australia) - 852 infected, 22 deaths and Diamond Princess (February | Japan) - 712 infected, 14 deaths. Coincidentally (or not), these outbreaks occurred on ships owned by Princess Cruises. Since 2003, the Princess has been part of the Carnival Corporation group, headquartered in theUnited States of America. The owner has 18 ships, most of which are registered in the Bermuda Islands (North Atlantic). The return operation return of their ships is scheduled for September 27, one of the most delayed among the other shipowners.
On May 15, the Princess Cruisesannounced dismissals, licences and wage and salary reductions for 50% of its workers in the cities of Santa Clarita (California) and Seattle (Washington), located on the west coast of the United States of America, due to the economic impacts generated by the pandemic.
Although the outbreak of COVID-19 contamination at Ruby Princess was the largest recorded in absolute numbers, the extensive literature of articles in international journals of infectology on COVID-19 outbreaks on ships gives greater prominence to the Diamond Princess - on which we will talk about in the next article - both because it was where the first outbreak happened, and also because it was the only one where it was possible to map the origin and evolution of the contamination, still inside the ship.